116 Thyroid cancer cases confirmed in Fukushima as of December 2015--100 in the first round and 16 in the second round (Total of 166 cases with malignancy or suspicion of malignancy--115 in the first round and 51 in the second round).
The 22nd Prefectural Oversight Committee for Fukushima Health Management Survey convened in Fukushima City, Fukushima Prefecture, on Monday, February 15, 2016.
(For the unofficial English translation of the most recent official information, only available in Japanese, on surgical and pathological details of some of the thyroid cancer cases, see this post).
Among other information, the Oversight Committee released the latest results (as of December 31, 2015) of the ongoing Full-Scale thyroid examination, or the second round screening, which is being conducted over a two-year period from April 2014 to March 2016. Although the so-called "final" results of Initial Screening, or the first round screening, were released at the last Oversight Committee meeting held on August 30, 2015, the secondary examination and surgical confirmation are still ongoing, and a few new additional results were orally presented.
An official English translation of the results is available here. The narrative below contains some information gathered from the live webcast of the Oversight Committee meeting and the subsequent press conference.
Overview
As of December 31, 2015, there are 14 more (2 from the first round and 12 from the second round) cases with malignancy or suspicion of malignancy, for a total of 166 (167 including the single case of post-surgically confirmed benign nodule). The number of surgically confirmed cancer cases, excluding the aforementioned case of benign nodule, now totals 116 (100 from the first round and 16 from the second round), and the remaining 50 (15 from the first round and 35 from the second round) await surgical confirmation. Since the last results were released, only 1 additional case from the second round has been operated on and confirmed as papillary thyroid cancer by post-surgical pathological examination of the resected thyroid gland tissue.
Initial (Preliminary Baseline) Screening (a.k.a. the first round)
The first round targeted about 368,000 individuals who were age 18 or younger, residing in Fukushima Prefecture at the time of the Tokyo Electric Fukushima Daiichi nuclear power plant accident on March 11, 2011. There were 300,476 actual participants in the primary examination, giving rise to the participation rate of 81.7%. As of December 31, 2015, there are 116 cases with malignancy or suspicion of malignancy, including a case of the post-surgically diagnosed benign nodule: 101 underwent surgery and 100 were confirmed with thyroid cancer (97 papillary thyroid cancer and 3 poorly differentiated thyroid cancer).
Full-Scale Screening (a.k.a. the second round)
To be conducted every 2 years until age 20 and every 5 years after age 20, the second round screening additionally targets those who were born in the first year after the accident, eventually aiming to examine approximately 385,000 individuals in a 2-year period. As of December 31, 2015, 236,595 have participated in the primary examination of the second round at the participation rate of 62.1% (target population as of December 31, 2015 is 381,261). 220,088 have received confirmed results of the primary examination, and 1,819 turned out to be eligible for the confirmatory examination.
Of 1,172 who actually underwent the confirmatory examination, 1,087 received confirmed results including 157 that underwent fine-needle aspiration cytology (FNAC). 51 cases had FNAC results suspicious for cancer. Confirmation of thyroid cancer requires pathological examination of the resected thyroid tissue obtained during surgery. As of December 31, 2015, 16 underwent surgery and all 16 were confirmed to have papillary thyroid cancer.
An additional new data from the first round
Dr. Akira Ohtsuru, the head of thyroid ultrasound examination program, orally presented information from the still ongoing secondary examination of the first round, mentioning 2 new cases with malignancy or suspicion of malignancy since the last results. There was no additional surgically confirmed cases. No details such as age, gender, or municipality of residence, are known about the 2 additional new cases with malignancy or suspicion of malignancy from the first round. It is also not known how many cases were still pending results of the confirmatory examination.
During the press conference, Asahi Shimbun jounalist Yuri Oiwa asked for age and gender of the two new cases from the first round. Otsuru declined to give the information, only stating that an addendum to the final report of the first round would be released at the next Oversight Committee meeting in May 2016.
Different age groups
In the first round, results are based on age at the time of the accident in March 2011 unless specified to be the age at examination. Age groups in the first round are shown in increments of 3 to 6 years from age 0 to age 18: 0-5, 6-10, 11-15, and 16-18. Meanwhile, age groups in the second round results are based on age at the time of examination, unless specified otherwise (Table 3 showing participation rates by age groups is based on age as of April 1, 2014). Age groups in the second round are shown in increments of 5 to 6 years from age 2 to age 23: 2-7, 8-12, 13-17, and 18-23.
Notably, the second round covers those who were born between April 2, 2011 and April 1, 2012: a cohort including those who were not conceived at the time of the accident and thus unexposed to the initial releases of radioactive iodine. Such cohort would yield valuable data of the unexposed population. This particular cohort also includes some who were already in utero, which also provides valuable data of in-utero exposure. Thus, the age 2-7 group in the second round includes both the in-utero exposed and the unexposed, but the breakdown of such data is not publicly available.
Incidentally, the reason for this time interval of April 2 to April 1 of the following year is the Japanese school year that starts in April: students born between April 2nd of the current school year and April 1st of the following year all enter the same grade. As thyroid ultrasound examination, like other school-based health checks and immunizations, has been taking place in school settings for school age children, officials decided to make sure students in the entire grade are "treated equally" so no children felt left out for having to or not having to go through the examination. (Conformity is considered a virtue in the Japanese society/culture, and any deviation can be a reason for bullying at any age, especially in children).
Newly diagnosed cases in the second round
In the second round, 12 cases were newly diagnosed by FNAC to be malignant or suspicious of malignancy. There were 5 males (age at exposure: 8, 8, 15, 16 and 18) and 7 females (age at exposure: 7, 10, 11, 11, 12, 12, and 14). Their places of residence at exposure include 6 municipalities: FY 2014 target municipalities such as Minamisoma City, Motomiya City and Koriyama City (5 cases); and FY 2015 target municipalities such as Iwaki City, Sukagawa City, Soma City, Nakajima Village, and Aizuwakamatsu City. (In the first round, Minamisoma City was included in the FY 2011 target municipalities; Motomiya City and Koriyama City in the FY 2012 target municipalities; and Iwaki City, Sukagawa City, Soma City, Nakajima Village and Aizuwakamatsu City in the FY 2013 target municipalities).
Prior diagnostic status of the cases newly diagnosed in the second round
Of 51 total cases with malignancy or suspicion of malignancy in the second round, 25 were A1, 22 were A2 (7 nodules and 15 cysts), and 4 were B in the first round. (In the 12 cases with malignancy or suspicion of malignancy reported this time, 6 were classified as A1, 4 as A2, and 2 as B in the first round).
In general, cysts are considered benign by nature due to their cell type unless they contain solid components which could contain malignant cells. In the protocol of Fukushima thyroid ultrasound examination, cysts with solid components are placed in the nodule category in the size range of the cysts themselves. Nodules, on the other hand, could be benign or contain malignant or pre-malignant cells.
25 cases that were A1 in the first round screened suspicious for malignancy in the second round. This would appear to be a new onset after the first round since A1 cases by definition have no ultrasound findings of cysts or nodules.
In 22 cases that were A2 in the first round, 7 were nodules and 15 were cysts. These 15 A2 cases with cysts, together with 25 cases that were A1 in the first round, represent 40 cases which developed thyroid cancer in 2 to 3 years since the first round. That is, unless these represented missed diagnoses.
According Ohtsuru, none of the cases had missed diagnoses in the first round. Otsuru did confirm during the press conference that there were no ultrasound findings for 25 cases that were A1 in the first round. However, he brought up a possibility that there might have been malignant cells already present at the time of the first round which could not be detected by ultrasound. (Medically speaking, this seems to be pure conjecture).
Ohtsuru also explained nodules would have to grow to be about 5 mm in diameter, or even 10 mm in some cases, to be detectible by ultrasound, although cysts could be detected beginning at 1 mm in diameter. However, this claim seems inconsistent with the long-standing claim by Fukushima Medical University that the ultrasound equipment being used is highly sensitive and capable of detecting very small lesions.
Ohtsuru seemed to be insinuating it was neither a missed diagnosis nor a new onset of cancer.
Unfortunately, Dr. Kazuo Shimizu, a thyroid surgeon and one of the committee members, was absent this time, and no meaningful medical discussion ensued regarding these "newly appearing cancers." Dr. Shimizu previously stated that although it would be difficult to assess whether these cancerous tumors occurred pre- or post-accident, information such as the previous diagnostic category--nodules or cysts--of the new cases with malignancy or suspicion of malignancy might give some clue as to whether the cancer appeared after radiation exposure.
Of 4 cases that were B in the first round, 2 were reported to have undergone FNAC in the first round, although the first FNAC results were undisclosed.
First Round or Initial Screening (October 2011 - April 2015)
Number of cases with malignancy or suspicion of malignancy: 116 (including one case of benign nodule)
Number with confirmed tissue diagnosis after surgery: 101
- 1 benign nodule
- 97 papillary thyroid cancer
- 3 poorly differentiated cancer
Second Round or Full-Scale Screening (April 2014 - March 2016)
Total number targeted: 381,261
Number of participants in primary examination: 236,595
Number with confirmed results: 220,088
- A1 89,565 (40.7%) (no nodules or cysts found)
- A2 128,704 (58.5%) (nodules ≦ 5.0 mm or cysts ≦ 20.0 mm)
- B 1,819 (0.8%) (nodules ≧ 5.1 mm or cysts ≧ 20.1 mm)
- C 0 (0.0%) (requiring immediate secondary examination)
(Note: Cysts with solid components are treated as nodules).
Number eligible for confirmatory (secondary) examination: 1,819
Number of participants in confirmatory examination: 1,172
Number with confirmed results: 1,087
Number of FNAB: 157
Number of cases with malignancy or suspicion of malignancy: 51
Number with confirmed tissue diagnosis after surgery: 16- 16 papillary thyroid cancer
Unofficial translation of the selected tables from Full-Scale screening
Table 1. Primary examination coverage as of December 31, 2015

Table 2. Number and proportion of children with nodules/cysts as of December 31, 2015

Table 3. Participation rates in target municipalities for FY 2014 by age group as of December 31, 2015

Table 4. Changes in the results of Initial Screening and Full-Scale Thyroid Screening Program as of December 31, 2015

Note 1: Top line refers to the results of the Preliminary Baseline Screening for confirmed results of the Full-Scale Screening.
It is not the breakdown of the total Preliminary Baseline Screening results, 300,476.
Note 2: Top line refers to the breakdown of the Full-Scale Screening results in a given category of the Preliminary Baseline Screening results.
Bottom line shows the proportion in %.
Table 5. Confirmatory testing coverage and results as of December 31, 2015

Table 6. Cytology results (including information from Appendix 6: Number of surgeries among cases with malignancy or suspicion of malignancy) as of December 31, 2015

Figure 3. Distribution of cases with malignancy or suspicion of malignancy by age (as of March 11, 2011) and sex (females in white and males in gray)

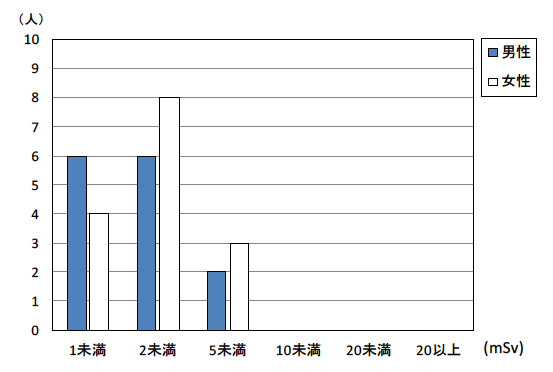
Figure 5. Estimated external effective doses of those who submitted basic survey questionnaire as of December 31, 2015 (females in white and males in blue)